Innovation in Specialty Medicine: a Pipeline to Watch Closely
July 18, 2022

Quick, a plumber! The specialty medicine pipeline is bursting. Medicines that could have been lifted from sci-fi novels are on their way to clinics, hospitals, and pharmacies throughout Canada. While R&D is flourishing in many therapeutic areas, data analysts have teased out oncology, neurology, and immunology as key drivers of innovation.11
All this is both exciting and daunting. There’s nothing simple or economical about these new medications, which require a complex infrastructure to support them. For example, patients may need sophisticated tests, including genetic analyses, to find out if a treatment is suitable for them. Once on the drug, they may need a battery of tests to ensure the drug remains a good fit.
How will the Canadian infrastructure handle this brave new pipeline? All signs suggest that stakeholders are ready to ride the wave of innovation and rise to the challenges along the way.
EXCITING TREATMENT AREAS TO WATCH
Oncology
Rare cancers, advanced cancers, cancers previously considered untreatable… scientists are working on treatments for them all. Indeed, cancer alone accounts for over a third (37%) of the specialty drug pipeline.4 That’s 2,226 cancer products in current development.4 Canada alone saw 17 new cancer drugs approved in the first half of 2021, a significant jump from the 15 that received approval in all of the previous year.5 Globally, the 5 years leading up to 2026 will usher 100 new oncology treatments into the toolbox, pushing the oncology drug market over the $300-billion mark.1
Even less prominent areas of oncology, such as kidney cancer, are welcoming new treatments every year. At the same time, researchers are moving beyond organ-based categories like “kidney cancer” or “lung cancer,” having discovered that the genomic characteristics of a tumour matter more than its location in the body. This insight has spurred the development of tumour-agnostic therapies, which target a tumour’s genomic profile, rather than its morphology or site.
Traditionally, oncology clinical trials have focused on patients with the most urgent needs, namely those with advanced cancers. This is changing: the past decade has seen a nearly two-fold increase in early cancer and cancer vaccine trials, with almost 200 trial starts in 2021—11% of the total for oncology.10
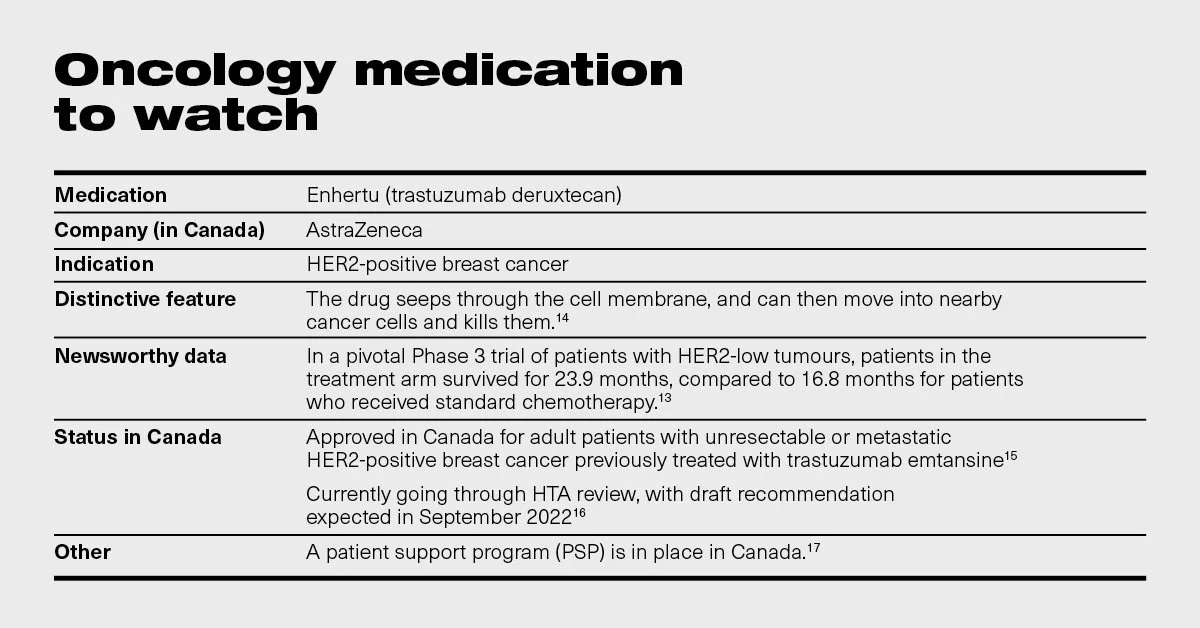
Innovation in advanced cancer treatment still dominates the scene, though, with superstars like HER2-positive breast cancer drug Enhertu grabbing headlines. Results of pivotal Enhertu trials showed a 49% reduction in disease progression as well as a 7-month survival advantage over chemotherapy in patients with hormone-receptor-positive and HER2-low tumours,12 which experts viewed as “stunningly successful.”13 In an interview for the New York Times, Dr. Halle Moore, director of breast medical oncology at the Cleveland Clinic, said “it is unheard of” for a metastatic breast cancer drug to improve survival to this extent, adding that “few people expected the drug to work [in HER2-low tumours] because other drugs for such cancers had failed.”13
Cell and gene therapy
Cell and gene therapies have brought the future to our doorstep. These advanced technologies target disease at its most basic source: defective genetic material. This means we can now think of curing, rather than merely treating, chronic diseases.
While the strategy of transferring healthy cells to a patient has a long history—the first bone marrow transplant occurred more than 50 years ago—recent advances have made it possible to reprogram cells to help the body repair itself.18 Gene therapies operate on a similar principle, though the transferred material consists simply of repaired genes, rather than whole cells.18 And some treatments, such as stem cell transplantation following genetic modification, combine both approaches.19
Over the past two decades, the discovery of several genes responsible for disease-causing mutations has injected new life into the cell and gene therapy market. As of May 2021, the pipeline had 1,745 therapies at various stages of development.20
TERMS OF THE TRADE: The lexicon of cell and gene therapy
Gene therapy: A technique for the treatment of genetic disease, involving replacement of a missing or defective gene with a healthy gene.3
Cell therapy: Transfer of live cells to a patient to help cure or treat a disease. The cells may come from the patient (autologous cells) or a donor (allogeneic cells).19
CAR-T therapy: A type of cell therapy that uses modified T cells to fight cancer.21 A patient’s T cells are collected and modified to produce chimeric antigen receptors (CARs) on their surface. These new receptors latch on to antigens on tumour cells and kill them.
Gene editing: Technologies such as CRISPR and TALON, which modify (edit) DNA.22 They can be used to induce T-cells to produce the CAR receptors needed for CAR-T therapy.
RNA therapy: While gene therapies make changes to DNA, RNA therapy alters the RNA in people with genetic diseases.23 The corrected RNA is then used to create the protein that was missing or defective.
Oncology remains the most active locus of cell and gene therapy research, with more than 1,300 candidate products in development,20 but these therapies also find niches in such areas as cardiovascular disease, respiratory disease, dermatology, neurology, and rare diseases, to name a few.20
One of the most prominent success stories in cell therapy, called CAR-T, involves manipulating cancer patients’ immune cells to turn them into cancer-killing cells. Especially effective for lymphomas and leukemias, this disruptive technology offers lasting remission to some cancer patients previously considered terminal—patients such as Emily Whitehead, one of CAR-T’s first success stories. Diagnosed with leukemia when she was just 5 years old, Emily, who lives in Pennsylvania, relapsed twice and her disease became resistant to treatment. Her only hope was CAR-T, and it didn’t disappoint: Now a vibrant teenager, Emily has been cancer free for over 10 years since her treatment, which made headlines globally.24
Canada has also been ushering in new CAR-T treatments—a notable example being Abecma, which received Health Canada approval in May 2021.3 The first CAR-T therapy approved for multiple myeloma (MM), Abecma modifies a patient’s blood cells to attack MM cells that express a specific antigen called BCMA, as do nearly all MM cells.25 While CADTH gave Abecma a “do not reimburse” recommendation in February 2022, citing insufficient evidence about duration of response and survival as a rationale,26 the medication finds itself on many “to watch” lists, including Canada’s own Meds Entry Watch.3
“One and done” treatments such as Abecma disrupt traditional care pathways and pharmaceutical business models. Scaling such treatments to generate sustainable value in Canada will require some new thinking.

In the meantime, Canadian researchers have been conducting their own cell and gene therapy R&D. An exciting case in point: Massimiliano Paganelli, head of the liver tissue engineering and cell therapy lab at Montreal’s Sainte-Justine children’s hospital, and his stem-cell biologist wife, Claudia Raggi, have developed a cell therapy for children with liver disease.29 They launched a biotech company, Morphocell Technologies, to test and commercialize the product, which they hope to deliver to patients within 2 years.29
Neurology
We’re playing with a double-edged sword: life expectancy has shot up over the past century, but advanced age – one of the major risk factors for neurodegenerative disorders – compounds the opportunities to develop such diseases as Alzheimer’s, Parkinson’s, stroke, and amyotrophic lateral sclerosis (ALS).30 Isabelle Aubert, a senior scientist at Sunnybrook Research Institute and Canada research chair in brain repair and regeneration, foresees a “tsunami of aging disorders” in the years to come.30
The most common of these disorders, Alzheimer’s, affects one in 9 people over age 65 and one in 3 over 85.31 More than 500,000 people currently live with Alzheimer’s and other forms of dementia in Canada, and if current trends continue, dementia will affect over 900,000 Canadians by 2030.9 With such figures looming ahead, it’s hardly surprising that scientists have doubled down on the search for effective treatments. The area has proven itself extraordinarily difficult to master, however, and after over 300 failed trials across the industry,32 many companies have pulled out.
The meteoric rise and fall of the drug Aduhelm in the U.S. exemplifies the turbulence of Alzheimer’s research. After a contentious accelerated FDA approval in June 2021, based on the surrogate endpoint of reduction in amyloid plaque,33 the product languished in the rollout phase. Unconvinced by the data, many physicians and major medical institutions refused to support it.34 Following suit, some insurers said they wouldn’t cover it. In reaction to these developments, manufacturer Biogen made the decision to “substantially eliminate” its marketing budget for Aduhelm.35
Even so, things are looking up for Alzheimer’s treatments, largely because clinicians can now diagnose the condition at a molecular level. “For so many years, we could not diagnose it until someone died,” notes Sara Manning Peskin, assistant professor of clinical neurology at the University of Pennsylvania and author of the book A Molecule Away From Madness. “Now we have the tools that we can pick up in living people, [namely] the proteins linked to Alzheimer’s,” she says.36 This technological advance has “opened up huge doors for clinical trial drugs for Alzheimer’s disease.”
“For many years, we couldn’t diagnose Alzheimer’s until someone died. Being able to identify Alzheimer’s in living people has opened up huge treatment doors.”
Pivotal trials are under way for ganenterumab, a monoclonal antibody for Alzheimer’s and one of the most anticipated medications of 2022. The ongoing 4-year Skyline trial will test the new dose in both patients with early Alzheimer’s and in those without symptoms but with evidence of plaque accumulation in the brain.37

Promising diseases under the neurology umbrella also include Parkinson’s and migraine, both common conditions with significant unmet needs. Many people with migraines are unable to use or tolerate currently available treatments, and the disease burden remains high even in those receiving migraine-specific medications.39 With Parkinson’s disease, the greatest unmet need lies in symptomatic motor control.40
Here in Canada, innovation in neurology just got a boost with new research collaboration between the Montreal Neurological Institute-Hospital, Takeda Development Center Americas, and Roche. The initiative will harness patient data toward the search for promising targets for neurologic drug development.41
Immunology
A handful of diseases involving the immune system, such as psoriasis, atopic dermatitis, and asthma, have been driving innovation in immunologic treatments. In the 5-year lead-up to 2026, the market is expected to grow by 39%.1
Many of the new treatments for auto-immune disorders are biologics—drugs derived from living material that interrupt faulty signals in the immune pathway. A noteworthy new product in this class, Tezspire, takes aim at the severe form of asthma, which affects 10% of people with the disease.42
The strength of the biologic market speaks to the unfortunate prevalence of auto-immune diseases in Canada. Asthma alone impacts more than 3.8 million Canadians, including 850,000 children under age 14, making it the country’s third most common chronic disease.43 Over 300 Canadians receive an asthma diagnosis every day, and asthma attacks kill an estimated 250 Canadians every year.43

The only direction for this market is up, not least because of the steady flow of biosimilars –molecules designed to work like a previously approved biologic – into the mix. Even before an originator biologic loses exclusivity, manufacturers begin working on matching biosimilars, ready to launch them when the patent protection expires. Three of the top-earning biologics in Canada – Remicade, Humira and Lucentis – have already passed through this stage, with Eylea and Stelara next in line.47 Because biosimilars cost less to develop, they create savings that can be reinvested into innovative new drugs. The next few years should prove very interesting.
ADAPTING TO THE INFLUX
R&D is just one step in the circle of specialty drug innovation. To complete the circle, stakeholders need to lay down the infrastructure to support new treatments and ensure their sustainability. Suzanne McGurn, CEO of CADTH, welcomes the challenge. “What could be more exciting than figuring out how we distill the promise of these drugs?” she said in an interview with Global Forum, adding that “the HTA process is about providing people with information to decide whether and what to buy, and sometimes it’s also about helping them prioritize who should get what and when.”48“What could be more exciting than figuring out how we distill the promise of these new treatments?”
As an example of infrastructure innovation, Canada is stepping up to bring CAR-T therapy to patients in need. Dr. Kevin Hay of the Vancouver Coastal Health Research Institute and his colleagues have received funding to build a Canadian CAR-T manufacturing network and transfer their know-how to other cities.49 In fact, Toronto and Winnipeg are developing the capacity to manufacture CAR-T cells. The complexities of CAR-T require national collaboration and dedicated centres of excellence, and the collective interest in getting such centres up and running bodes well for the future of CAR-T in Canada.
Patient support in flux
In step with such creative collaborations, the patient support program (PSP) ecosystem will need to accommodate the new generation of specialty medicines. PSPs for oncology drugs alone currently hover at 175,50 and the number of PSPs continues to rise every year. What’s more, most existing PSPs support relatively small patient populations—by one industry expert’s estimate, no more than 30,000 and often well below that figure.11 With the market poised to introduce specialty drugs that serve much larger populations, manufacturers and the specialty service providers that support them will need to develop PSPs that can effectively serve these broader and more varied groups.
Technology can help in this regard, enabling the design of more flexible programs that allow patients to customize their PSP journey. For example, today’s PSP may have a nurse calling every patient at predetermined intervals. The PSP of tomorrow may enable patients to “choose their own adventure”—their preferred method, frequency, and style of communication.
This flexible, patient-centred philosophy must also extend to caregivers, who play an indispensable role in managing high-need groups such as children, cancer patients, and people with dementia. Indeed, the usual trajectory of dementia has a caregiver stepping up to manage the patient, and as many as 20% of Canadians have experience caring for someone with dementia.9 Stakeholders increasingly recognize the caregiver journey as integral to the treatment experience, and many PSPs include caregivers in their offerings. Future PSPs have an opportunity to build on this approach to address an expanding array of caregiver needs. As treatments become increasingly complex, the PSP paradigm may even shift from the individual patient and caregiver to the family unit. For example, a PSP could assist a family that needs to accompany a patient travelling for an infusion, or provide mental health services to help a family cope with the stress of a taxing treatment protocol.
Physicians, for their part, will need to adapt to a prescribing landscape dotted with PSPs. With specialty drugs now entering therapeutic areas historically reserved for general medicine, many specialists who don’t currently deal with PSPs will need to learn the ropes. For example, prostate cancer, an area traditionally treated by in-hospital oncologists, is increasingly falling to urologists to manage. With all the specialty migraine drugs entering the market, neurologists may face similar pressures. PSP program administrators will need to educate these clinicians about the nuances of the specialty medicine ecosystem to ensure their patients don’t miss vital opportunities for clinical support, prior authorization, or co-pay assistance.
Brave new data
Big drugs require big data. Real-world data (RWD) sources such as health-system records and registries can help manufacturers identify the patient population served by a treatment and find out what they’re currently missing. In practice, this can pose challenges. For example, current administrative data sets do not code “mild cognitive impairment” as dementia,11 making it harder to track down candidates for an early-dementia treatment without resorting to labour-intensive chart reviews. Likewise, current data sets do not readily distinguish chronic from episodic migraine patients.11
With regulators and payers insisting on increasingly robust evidence to support approval and listing, manufacturers will need to create data plans that span several years – including prior to drug launch. This endeavour may call for creative partnerships, such as the December 2021 agreement between Janssen Research & Development and EVERSANA, a provider of next-gen data services to the life sciences industry. The collaborators will mine data from EVERSANA’s chronic disease database, which covers more than 80 million patients, to help enhance clinical trial design and assess how therapies perform in real-world settings.51
Data also offers a path toward greater treatment equity. For example, clinical trial data has uncovered the uncomfortable truth that Black people represent only 2% of subjects in Alzheimer’s clinical trials, despite developing the disease at higher rates than Caucasians.52 As the industry zooms in on real-world performance, we have a responsibility to use data to characterize real-world diversity and recruit subjects that reflect it.
The way forward
As the curve of innovation continues to rise, the specialty drug ecosystem will need to evolve apace. Stakeholders throughout the world are setting up new processes to shorten the time to specialty drug access, giving Canada the means to follow suit.
One such initiative, a collaborative global program called Project Orbis, has already made strides toward its goal of accelerating access to innovative cancer treatments. Last year, the program helped fast-track a medication called Tagrisso toward regulatory approval for a new indication – early stage non-small-cell lung cancer – and listing on the same date in the UK.53 Here in Canada, one of Project Orbis’s participant countries, the trek to Tagrisso access hasn’t gone quite as quickly: while the new indication received approval in early 2021, the listing application remains in “active negotiation” status at the pCPA as of mid-2022.54
As the above case exemplifies, access will likely pose a challenge for some time to come, especially for therapies that show promise but have limited evidence and a high degree of budget uncertainty. The pipeline abounds with such medications, offering new hope to patients—but only if they can access the drugs. As the innovative specialty medicine pipeline evolves, stakeholders will need to explore innovative approaches that harness real-world evidence to mitigate risk. Specific strategies and tools may change as the pipeline diversifies, but the goal remains the same: the right medicine to the right patient at the right time.
References
1. The global use of medicines 2022, outlook to 2026. IQVIA. https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/the-global-use-of-medicines-2022/global-use-of-medicines-2022-outlook-to-2026-12-21-forweb.pdf
3. Meds pipeline monitor 2021. Patented Medicine Prices Review Board. https://www.canada.ca/content/dam/pmprb-cepmb/documents/npduis/analytical-studies/meds-pipeline-monitor/2021/Meds-Pipeline-Monitor-2021-EN.pdf
4. Global trends in R&D 2022. IQVIA. Feb. 10, 2022. . https://www.iqvia.com/insights/the-iqvia-institute/reports/global-trends-in-r-and-d-2022
5. Mid-year update. Health products approved in 2021. Government of Canada. https://www.canada.ca/en/health-canada/services/drugs-health-products/highlights-reports/mid-year-update-2021.html
9. Dementia numbers in Canada. Alzheimer Society. https://alzheimer.ca/en/about-dementia/what-dementia/dementia-numbers-canada
10. Global oncology trends 2022, outlook to 2026. IQVIA. https://www.iqvia.com/-/media/iqvia/pdfs/institute-reports/global-oncology-trends-2022/iqvia-institute-global-oncology-trends-2022-forweb.pdf
11. 20Sense original research.
12. ASCO22: Enhertu halves risk of disease progression in HER2-low breast cancer study. FirstWord Pharma. June 5, 2022. https://firstwordpharma.com/story/5587727
13. Breast cancer trial results in ‘unheard of’ survival. New York Times. June 7, 2022. https://www.nytimes.com/2022/06/07/health/enhertu-breast-cancer-chemotherapy.html
14. Breast cancer trial results in ‘unheard of’ survival. New York Times. June 7, 2022. https://www.nytimes.com/2022/06/07/health/enhertu-breast-cancer-chemotherapy.html
15. ENHERTU product monograph. AstraZeneca Canada. Nov. 19, 2021. https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/enhertu-product-monograph-en.pdf
16. Trastuzumab deruxtecan. CADTH. Last updated June 10 2022. https://www.cadth.ca/trastuzumab-deruxtecan
17. Trastuzumab deruxtecan. Canadian Breast Cancer Network. https://cbcn.ca/en/listing-directory/drug-navigation-tool/trastuzumab-deruxtecan
18. Cell and gene therapy: the next milestone in fighting diseases. Bayer Global. https://www.bayer.com/en/news-stories/cell-and-gene-therapy
19. Cell and gene therapy FAQs. American Society of Cell + Gene Therapy. https://asgct.org/education/more-resources/gene-and-cell-therapy-faqs
20. Gene, cell, & RNA therapy landscape. American Society of Cell + Gene Therapy. https://asgct.org/global/documents/asgct-pharma-intelligence-quarterly-report-july-20.aspx
21. Frequently asked questions about CAR-T cell therapy. Dana-Farber Cancer Institute. https://www.dana-farber.org/cellular-therapies-program/car-t-cell-therapy/faq-about-car-t-cell-therapy/
22. CAR-T cells: engineering patients’ immune cells to treat their cancers. National Cancer Institute. https://www.cancer.gov/about-cancer/treatment/research/car-t-cells
24. Our journey. Emily Whitehead foundation. https://emilywhiteheadfoundation.org/our-journey/
25. Frequently asked questions: Abecma. Cancer Connect. https://news.cancerconnect.com/treatment-care/frequently-asked-questions-about-abecma-idecabtagene-vicleucel-ide-cel
26. CADTH reimbursement recommendation: Abecma. https://www.cadth.ca/sites/default/files/DRR/2021/PG0240%20Abecma%20-%20CADTH%20Final.pdf
27. Abecma product information. Bristol Myers Squibb. https://www.abecma.com/
28. How was Abecma studied? Bristol Myers Squibb. https://www.abecma.com/abecma-treatment-outcomes/abecma-results/
29. Canada should be manufacturing its own cell and gene therapies, not just vaccines. The Globe and Mail. April 12, 2022. https://www.theglobeandmail.com/business/commentary/article-canada-should-be-manufacturing-its-own-cell-and-gene-therapies-not/
30. Toronto researchers are on a quest to end brain disorders. MaRS. Feb. 22, 2022. https://www.marsdd.com/news/toronto-researchers-are-on-a-quest-to-cure-brain-disorders/
32. An Alzheimer’s treatment fails: ‘We don’t have anything now.’ New York Times. Feb. 10, 2022. https://www.nytimes.com/2020/02/10/health/alzheimers-amyloid-drug.html
33. FDA approves Biogen, Eisai's Alzheimer's therapy Aduhelm. FirstWorld Pharma. June 7, 2021. https://firstwordpharma.com/story/5319993
34. Clinics won’t provide it. Insurers won’t cover it. So will the first Alzheimer’s drug make a difference? Time. Aug. 5, 2021. https://time.com/6081333/biogen-alzheimers-drug-aduhelm-fda-controversy/
35. Biogen caves in on Aduhelm: how Alzheimer’s disease biotechs can avoid similar mistakes. Clinical Trials Arena. May 5, 2022. https://www.clinicaltrialsarena.com/news/biogen-caves-in-on-aduhelm-how-alzheimers-disease-biotechs-can-avoid-similar-mistakes/
36. The science behind mental afflictions. The Book Review (New York Times podcast). March 18, 2022. https://open.spotify.com/episode/1cjLPCTKm4sl8MuqnPWgtB
37. Roche plans 4-year late-stage trial for Alzheimer's candidate while awaiting crucial H2 readout. Fierce Biotech. March 3, 2022. https://www.fiercebiotech.com/biotech/roche-plans-4-year-study-alzheimers-med-gantenerumab-once-failed-drug-has-key-2022-readout
38. Klein G et al. Alzheimer’s Research & Therapy 2019;11:101.
39. Mallick Searle T, Moriarty M. J Am Assoc Nurse Pract 2020;33:419.
40. LeWitt PA, Chaudhuri KR. Parkinsonism Relat Disord 2020 Nov;80 Suppl 1:S7-S12.
41. Academia and industry collaborate to find new targets for neurological disease treatment. Neuro. Feb. 3, 2022. https://www.mcgill.ca/neuro/channels/news/neuro-genomics-partnership-aims-drive-neurological-disease-research-337384
42. Top ten most anticipated drug launches of 2022. Fierce Pharma. Feb. 7, 2022. https://www.fiercepharma.com/special-report/10-most-anticipated-drug-launches-2022
43. Understanding Asthma. Asthma Canada. https://asthma.ca/get-help/understanding-asthma/
44. FDA approves Tezpire in the US for severe asthma. Amgen. Dec. 17, 2021. https://www.amgen.com/newsroom/press-releases/2021/12/fda-approves-tezspire-tezepelumabekko-in-the-us-for-severe-asthma
45. New Tezepelumab data show 86% reduction in exacerbations in patients with severe asthma and comorbid nasal polyps. Cision PR Newswire. Sept. 5, 2021. https://www.prnewswire.com/news-releases/new-tezepelumab-data-show-86-reduction-in-exacerbations-in-patients-with-severe-asthma-and-comorbid-nasal-polyps-301368866.html
46. New drug submissions under review. Government of Canada. https://www.canada.ca/en/health-canada/services/drug-health-product-review-approval/submissions-under-review/new-drug-submissions-under-review.html#tbl1
47. The top 15 blockbuster patent expirations coming this decade. Fierce Pharma. July 12, 2021. https://www.fiercepharma.com/special-report/top-15-blockbuster-patent-expirations-coming-decade
48. Changing landscape of evidence charting new assessment pathways. Global Forum. https://globalforum.diaglobal.org/issue/october-2021/changing-landscape-of-evidence-charting-new-assessment-pathways/
49. A Canadian first in CAR-T cell treatment for adult leukemia and lymphoma. Vancouver Coastal Health Research Institute. Aug. 31, 2021. https://www.vchri.ca/stories/2021/08/31/canadian-first-car-t-cell-treatment-adult-leukemia-and-lymphoma
50. Manufacturer patient assistance programs. BC Cancer. June 2022. http://www.bccancer.bc.ca/systemic-therapy-site/Documents/Policy%20and%20Forms/Patient%20assistance%20programs.pdf
51. EVERSANA announces real-world data agreement with Janssen to augment development of chronic disease care therapies. Eversana. Dec. 16, 2021. https://www.eversana.com/2021/12/16/eversana-announces-real-world-data-agreement-with-janssen-to-augment-development-of-chronic-disease-care-therapies/
52. Alzheimer’s trials exclude black patients at ‘astonishing’ rate. Bloomberg. April 19, 2022. https://www.bloomberg.com/news/articles/2022-04-19/drug-trials-are-more-likely-to-admit-white-people
53. AstraZeneca secures license extension and early NHS England access to Tagrisso. Pharmiweb. May 7, 2021. https://www.pharmiweb.com/press-release/2021-05-07/astrazeneca-secures-license-extension-and-early-nhs-england-access-to-tagrissotm-osimertinib-for-patients-with-completely-resected-early-stage
54. Tagrisso (osimertinib). pan-Canadian Pharmaceutical Alliance. https://www.pcpacanada.ca/negotiation/21713