Evaluating the Impact of Drug Access Initiatives
April 24, 2025

Are Canadian drug access initiatives really delivering for patients?
As the specialized drug pipeline continues to flow hard and fast, patient access has taken on an increased urgency in Canada. The need to expedite access to life-changing therapies has led to new policies, new pathways, and new pilot projects. Now come the hard questions: Are the initiatives working as intended? Are they truly enabling timelier and more equitable access for Canadian patients? As we will see in this article, we can’t shout “yes” from the rooftops yet.
PATIENT ACCESS IN CANADA TODAY
Canadians wait up to two years, and occasionally even longer, before they can access new Health Canada-approved treatments through public health plans – if at all. In this regard, Canada ranks 19th out of 20 OECD countries and last in the G7.2 In 2024, the time from regulatory approval (or notice of compliance [NOC]) to first provincial listing was 598 days.2 While this shows improvement from the previous year (677 days), in 2020 the corresponding time was 541 days, or 57 days less than the 2024 figure. Bottom line, the collective efforts undertaken between 2020 and 2024, however laudable, did not shorten the time to access within public drug plans.1
Average time from NOC to first provincial listing, 2020-2024 (in days)
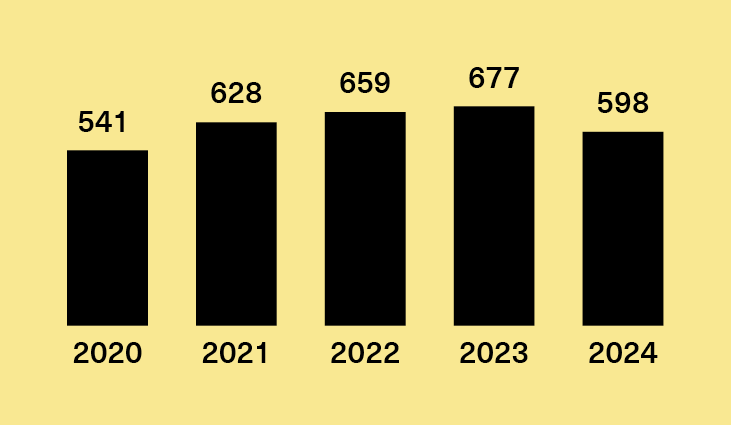
Source: IQVIA Market Access Metrics, December 2024. All products with CDA-AMC review were included.
“Just as we've observed in the public payer side for years, our private access metrics now reflect a growing trend in time to listing,” says Brad Millson, IQVIA’s General Manager, Real World Solutions, adding that “in the last couple of years we've seen examples of certain drugs taking upwards of 2 years to gain coverage on some private plans.”
This unpredictable state of affairs leaves patients understandably frustrated. While painfully aware of the Health Canada-approved medications that could change their lives, they often can’t break through the access wall. As Glenn Hussey, a retired public servant and multiple myeloma patient in Ottawa, puts it, “it gets very frustrating for patients when they see everything that's there and they cannot yet get access to it.”8 According to Dr. Sandy Sehdev, an oncologist at the Ottawa Cancer Centre, physicians experience complex emotions of their own. It “causes us great anguish when we have a drug we know will help [patients] that we can't get for them,” says Sehdev, who lays much of the blame at bureaucracy’s sluggish feet.8
Most stakeholders would agree that timely access can have benefits for the patient – and for health systems at large. Consider cystic fibrosis (CF), a rare genetic disease that impacts the lungs and other internal organs. In 2021, a life-changing new treatment option for CF, Trikafta, received NOC from Health Canada. For the more-than-4,000 Canadians living with CF, the drug promised a significant decrease in the need for acute care. Indeed, in the year after patients began taking the medication, hospitalizations decreased by 65%, emergency visits dropped by 20%, and use of antibiotics for acute infections went down by 58%.6
Such encouraging figures notwithstanding, egregious access barriers and inequities persist. Let’s start with the great unequalizer, postal code. In Quebec, adult patients with spinal muscular atrophy (SMA), a motor neuron disease that affects basic activities like walking and swallowing, can access novel disease-modifying medications; if they live elsewhere in Canada, they’re out of luck.9 And while they wait for a policy change that would put them on par with their provincial neighbours, their disease continues to progress. It’s no wonder that some of them, like Ontario hobby farmer Bryan Weatherall, ask themselves: “Why not me?”9
In British Columbia, meanwhile, a 9-year-old girl with Batten disease, a rare condition that causes seizures and motor loss, received notification from the public drug plan that her drug treatment would be cut off. Just days later, in a whiplash-inducing about-face, the government decided to continue to offer the $1M treatment while reviewing the file.10,11 Access calamity averted – for now.
Geographical arbitrariness also prevails within cancer treatment. In Ontario, cancer patients can obtain IV medications without cost or delay. If their therapy consists of take-home pills – which are much less burdensome on the healthcare system and the patient – however, they face steep costs and weeks or months of waiting before they can begin treatment.12 Most other provinces have created mechanisms to speed up access to oral cancer drugs, leaving Ontario more than a decade behind the times.
AWARE OF THE PROBLEM
The need for faster and fairer access has not escaped policymakers. In the opening session of Canada’s Drug Agency (CDA-AMC)’s September 2024 conference in Ottawa, Suzanne McGurn, CDA-AMC’s president and CEO, articulated the imperative to “improve our systems [so] that patients will be able to see that they’ve gotten medicines faster.”13 To this end, she pledged to strengthen CDA-AMC’s role as a convenor “to bring our partners together to strengthen the system, while we continue to deliver the high-quality evidence that stakeholders depend on.”
Speaking at the same conference, Patrick Dicerni, who holds deputy minister and executive officer positions at the Ontario Ministry of Health and Long-Term Care, affirmed that “I never like to be last at anything or bottom quartile of anything. If we look at time to access, if you’re in the bottom of the OECD countries, I see an opportunity for us to move up that ladder with good coordination.” Echoing the sentiment at a news conference last year, Ontario Premier Doug Ford noted that Canada currently ranks last in the G7 in terms of drug approval/access time and proclaimed that “this needs to change.”14
“I never like to be last or in the bottom quartile of anything. I see an opportunity for Canada’s access times to move up the OECD ladder with good coordination.”
Patrick Dicerni
Assistant Deputy Minister, Health Programs and Delivery Division,
Ministry of Health, Ontario Public Service
Likewise, the pan-Canadian Pharmaceutical Alliance (pCPA), which conducts collective negotiations with drug makers on behalf of public drug plans, “recognizes the need for timely patient access to treatments and works to balance the need for early access with availability of sufficient evidence.”15 But how? As a start, the pCPA has recently offered up one new pathway to “establish a unique process and funding mechanism where patients, physicians and other stakeholders are made aware that coverage of the medication is temporary, conditional on manufacturer’s agreement to a risk-share arrangement, and subject to change dependent on subsequent evidence review.”15
Weighing in from the industry side, Amgen Canada notes that “less than 20 per cent of new medicines launched globally are available on Canadian public plans, and patients wait almost twice as long to access them compared to peer countries” and attributes this logjam to “Canada’s multi-layered, sequential system for public reimbursement.”16 For advanced treatments that address high unmet needs, Amgen views streamlined CDA-AMC and pCPA processes and innovative risk-sharing agreements as the path forward.16
THE IMPACT FACTOR
To gauge our progress along this path, let’s look at some major drug access initiatives currently happening in Canada: the national strategy for rare disease drugs, a proposed pilot project to cut access timelines by 9 months, CDA-AMC’s time-limited recommendation category, and INESSS’s “promise of value” HTA recommendation option. We’ll consider these initiatives through the lens of their impact on timely patient access to date.
Drug access initiatives: Measuring the impact on timely patient access, to-date
|
National strategy for rare disease drugs |
Minimal |
|
A provincially mandated pilot project to cut drug access time |
N/A – not yet launched |
|
CDA-AMC's time-limited recommendation category |
Minimal |
|
INESSS’s “promise of value” recommendation option |
Significant |
Initiative 1: National strategy for rare disease drugs
In March 2023, the federal government pledged to allocate $1.5 billion over three years for a National Rare Disease Drug Strategy.17 The bulk of those funds – about 1.4 billion – would go to the provinces through bilateral agreements, while $32 million was earmarked for research and $20 million for data collection. After a long delay, the bilateral agreements are finally in place.18 That’s great news, right?
Not quite: if we dig a little deeper, we find little evidence that the funds are creating optimal value for patients, health systems, and governments. According to the terms of the bilateral agreements, provinces need only fund a single drug from a short common list in the first 2 years19 – and most of the drugs currently on the list are already accessible to patients through the public drug plans.7 By year three, the agreements require the provinces to cover just 10% of the funding for the listed drugs.19 As Durhane Wong-Rieger, President & CEO of the Canadian Organization for Rare Disorders (CORD), sees it, “this equates to free money for the provinces.”7 Not just that, but the agreements do not require the money saved in provincial drug budgets to flow to rare diseases. In other words, “the agreements are not additive – they’re just shifting money from one budget to another, rather than providing additional funding for access to rare disease drugs.”
Another weakness in the framework: “Most drugs in the common list are already approved and recommended and have listing agreements in place,” says Wong-Reiger.7 In other words, the strategy does not help move novel advanced therapies through the system any faster – or reach patients any sooner. What also frustrates Wong-Reiger is that, two months after Ontario signed onto the strategy, the province has no plan to identify, diagnose, and refer and treat those patients with rare disorders.20 And if you’re a patient who happens to live in British Columbia, “you still have to appear individually in front of the rare disease committee to access these therapies.”7
On balance, CORD anticipates the $1.4 billion will yield “no net sustainable benefit for persons living with rare disease and their families, unless governments take a different course of action now.”21 To be clear, “CORD is “thrilled to have the funding [made available],” says Wong-Reiger.22 What’s missing are the “special pathways to make sure these funds get to people who need them.18
Even Beth Vanstone, a Beeton, Ont. rare disease patient advocate (and parent of a young woman with cystic fibrosis) and self-described “glass half-full kind of person,” has struggled to see the bright side of the national strategy in its current form. “It doesn’t come close to addressing the challenges that rare disease patients face,” she maintains.20 “The bilateral agreements are just another layer, the provinces cherry-pick what they want from the list, and the postal code lottery still exists. Patients don’t have the luxury of time – lives and limbs are being lost while they wait.”
“The national rare disease strategy doesn’t come close to addressing the challenges that rare disease patients face. Lives and limbs are being lost while they wait.”
Beth Vanstone
Rare Disease Patient Advocate
Impact factor to date: Minimal
Initiative 2: A provincially mandated pilot project to cut drug access time
In December 2024, Canada’s premiers called on the Ministers of Health to plan a pilot project to cut drug access time by 9 months.14 The framework they proposed would cover 7 to 10 cancer drugs approved by Health Canada through Project Orbis, a process for reviewing cancer drugs spearheaded by the FDA Oncology Center of Excellence initiative and adopted by several partnering jurisdictions, including Canada. 23 Between 2019 and 2024, Health Canada reviewed 74 approved cancer drugs through Project Orbis, averaging over 12 per year. 23 In Canada’s current drug access process, the various functions of each agency, including the drug price negotiation at the pCPA, happen in sequence. The pricing negotiation, which can begin after a positive CDA-AMC recommendation, has a target duration of 6.5 months. In 2024, however, the total negotiating time averaged 8.35 months – a significant delay to patient access – and only 35% of files achieved the target. 4 Within the proposed framework, drugs would be listed in the public plans – meaning patients would have access – as soon as they receive a positive CDA-AMC recommendation, with temporary agreements in place during pricing negotiations. This parallel process would save patients the 9 months that pCPA negotiations currently take.
A similar framework was deployed successfully in the UK in 2021-22, when 4 Project Orbis drugs got listed immediately after regulatory approval, with temporary early access agreements secured while the regular steps in the drug approval process were underway. The drugs in question, all treatments for non-small cell lung cancer, served small populations with a high unmet need. The framework shortened access by an average of 200 days, or 7 months. 7 Shifting our sequential process – HTA first, price negotiations second – to a parallel one would move us in the right direction, but patient advocate and health policy consultant Louise Binder suggests we go still further. “It can all happen at the same time: Health Canada approval, health technology assessment, and pricing negotiations,” she says. “Each agency looks at the same file through a different lens, with the whole process converging on a fair negotiated deal.”
Back to reality: the proposed accelerated oncology drug framework got a hearing at the January 2025 Federal Provincial Territorial Health Ministers' Meeting in Halifax, but the meeting’s summary statement on pharmaceutical management made no mention of the pilot project.24
Can we anticipate some movement on the file? We’ll be watching closely, as this initiative holds significant promise to enable timelier and more equitable access for cancer patients to novel therapies across Canada.
Impact factor to date: N/A – not yet launched
Initiative 3: CDA-AMC's time-limited recommendation category
Recognizing the “significant opportunities to improve our systems,” CDA-AMC’s Suzanne McGurn has pledged to bring promising new medicines to patients faster than before.13 To this end, CDA-AMC has proposed several innovative approaches, from supporting rare disease registries with real-world evidence (RWE) guidelines to conducting “rolling reviews” of novel therapies as soon as new evidence becomes available, rather than waiting for a complete submission package.25,26 The rolling review framework supports CDA-AMC’s Target Zero objective: achieving zero days between NOC and their draft HTA reimbursement recommendation.26
One of the most promising avenues for shortening the time to access is CDA-AMC’s time-limited recommendation (TLR) category, created to “provide earlier access to promising new treatments that target the unmet needs of people in Canada living with severe, rare, or debilitating illnesses.”27 Intended for advanced therapies that received a notice of compliance with conditions (NOC/c) from Health Canada, the TLR pathway dovetails with the pCPA’s temporary access process (pTAP), which informs pricing negotiations and possible listing agreements for drugs which receive a positive TLR.28 Together, these processes comprise the first made-in-Canada early access pathway – an important new chapter in the Canadian access story.
The combined TLR-pTAP pathway encountered its first test case in late 2023, when CDA-AMC granted a positive TLR recommendation to epcoritamab, a treatment for diffuse large B-cell lymphoma. Negotiations with the pCPA concluded in mid-2024, with provincial listings starting to appear a month later. The total time between NOC and listing, 306 days, significantly undercut the historical average of close to 600 days for oncology therapies.28
Despite this early success, only one more of the 7 drugs that has received NOC/c since that time has elected to enter the TLR-pTAP pathway. (The product is still undergoing review at the time of writing.) In an effort to understand the pain points and opportunities, CDA-AMC held consultations in early 2025. “What we heard overwhelmingly is that [the TLR pilot] should be expanded much more beyond the scope of what we initially put forward,” said CDA-AMC Director of Pharmaceutical Reviews Peter Dyrda in a recent webinar, adding that the organization is “open to proposals to see how we can expand the pilot if there’s a compelling case.”29
A recent analysis of the TLR-pTAP pathway identified opportunities to squeeze extra juice from the process, including expanding eligibility beyond NOC/c drugs, allowing more flexibility in the use of clinical-trial and real-world data, and disclosing the metrics used by CDA-AMC to evaluate TLR, such as number of patients impacted and access time achieved.7,28
A more ambitious expansion of TLR would enable the program to fulfill its promise and reach more patients in need. Stakeholders of all stripes are waiting to see how CDA-AMC adapts TLR to this opportunity.
Impact factor to date: Minimal
Initiative 4: INESSS’s “promise of value” recommendation option
The Quebec Life Sciences Strategy, published in 2017, counted faster access to high-value drugs and use of RWE among its objectives.30 Building on these aims, Quebec’s HTA agency, INESSS, created a recommendation option called “promise of value” in 2018. The designation seeks to facilitate conditional listings of medications that address high unmet needs, with the understanding that further monitoring and RWE will be required to support a more permanent listing.30 Since that time, approximately 10 files have received a positive recommendation within the promise-of-value pathway.7
The pathway’s value became evident in 2019, when it led to a positive recommendation for the SMA drug Spinraza, with continued coverage after the first year of treatment contingent on patient outcomes.31 Previously recommended only for children with a specific gene mutation, the drug now became available to adults with SMA. Three years later, CDA-AMC issued a negative recommendation for the adult indication of Spinraza, citing missing RWE and other limitations that “prevented the committee from concluding that [Spinraza] would fill the unmet needs expressed by patients and clinicians.”32 As such, adult patients outside of Quebec have not been able to access this drug through public drugs plans. One country, two HTA agencies, same evidence, two opposite outcomes.
A key milestone with the INESSS promise of value recommendation is the reassessment of the treatment in question on the basis of subsequent evidence, as happened for the first time with two drugs in the CAR-T class: Kymriah and Yescarta. For both these drugs, the initial conditional recommendation hinged on the collection of real-world data on duration of clinical response, subsequent treatments, and overall survival rates at 1 and 3 years.33,34 Upon reassessment in 2024, both drugs maintained a “positive with conditions” recommendation, with no change to the indication, and the “promise of value” codicil was removed.35,36
Of note, the evidence packages to support the reassessments included not just additional clinical trial data but supplementary RWE, some of it involving Canadian patients. For example:
- A 2023 retrospective analysis of 25 patients treated at CHU de Québec-Université Laval. 15 patients received Yescarta and 10 patients received Kymriah. The data was extracted from electronic patient records.37
- Unpublished data on patients across Canada from Hospital Maisonneuve Rosemont, provided either by the manufacturer or obtained directly from INESSS.38 For the reevaluation, INESSS restricted their analysis to patients in Quebec.7
These two drugs – the first CAR-T therapies approved in Canada – ushered in a new era of cancer treatment, and all stakeholders were learning as the use of CAR-Ts in the Canadian setting unfolded. To its credit, INESSS did not set the timeframe for re-evaluation in stone – for Kymriah it happened after 5 years, and for Yescarta 3.5 – and responded dynamically to the evolving treatment landscape. INESSS also showed leadership in leveraging Canadian RWE and trust in using it as a decision-making input.
The organization’s adaptability to the dynamic drug and treatment landscapes, rather than adherence to a rigid, preset process, facilitated evidence-based decision-making and supported access to critical treatments. It’s not perfect, but it sheds light on the mindset and methods required to impact patient access. Learnings from these first cases will help inform future use of this recommendation category and will also help to propel the access timeline to new levels of efficiency and equity for patients.
Impact factor to date: Significant
NOT THE END
The above-described initiatives have pointed us in the right direction, but much work remains to be done – starting with ruthless self-analysis. As a recent Healthy Debate article suggests, “we need to be OK with a relentless questioning of why quality of care isn’t evenly distributed across geographies, disease states and population groups.”39
Fortunately, the political will appears strong. At a November 2024 meeting of Life Sciences Ontario, speakers identified timely patient access to medications as a government priority, noted that timely patient access goes beyond funding decisions, and recognized the need to integrate the different administrative streams that culminate in access.40
Ultimately, stakeholder collaboration will be key to dislodging the administrative backlog in the system. Eva Villalba, executive director of the Quebec Cancer Coalition, gets right to the point: “I am haunted by a question asked by a patient with metastatic cancer: ‘Will I end up dying of bureaucracy?’ ”41
“I am haunted by a question asked by a patient with metastatic cancer: ‘Will I end up dying of bureaucracy?’”
Eva Villalba
Executive Director, Quebec Cancer Coalition
We have the political vision, resources, and responsibility to ensure this doesn’t happen. Let’s keep the ball rolling – patients are counting on all of us.
New Brunswick: Expanding the horizons for drug access
“If you take a look at where Canada sits globally in terms of accessing innovative medicine, there's a lot of work to be done.”42 That’s a key motivator for Jennifer Sheils, Vice President of Strategy, Transformation and Chief Innovation Officer at Horizon Health Network, the largest regional health authority and hospital system in New Brunswick. With the support of industry partners, they’re working on novel initiatives to get innovative medications to patients in a more timely and equitable way. “We believe that research is care,” said Jennifer. “It can give patients an opportunity they might not otherwise have, to get access to a breakthrough drug.”42
To support more equitable access to clinical trials and novel medications, Horizon mapped the patient journey in New Brunswick and found that many patients live outside urban areas, limiting their access to trials. They are now working on initiatives to involve more physicians in rural communities in their studies1 and they’ve recently created a network of university-affiliated hospitals to support those research efforts across the province.43
One of their core studies is designed to make care more accessible for patients with lung cancer. In partnership with Roche, Horizon will send nurses to patients’ homes to administer a subcutaneous immunotherapy. “Standard of care for many of these patients is an IV therapy, which means the patient has to drive in, maybe take a day off of work, maybe uproot their family,” said Jennifer. “So, we wanted to empower patients with a choice: rather than coming to the hospital, they could have an injection at home.” In addition to improving the patient experience, Horizon hopes this will reduce hospital resource use.42,44 Horizon is also developing an alternate pathway for oncology drug access, whereby Amgen will provide therapies to network sites directly. This program will run in parallel with the existing listing process, while dramatically reducing patients’ waiting time for innovative treatments.45
Jennifer hopes that Canada can learn from timely access initiatives in the EU and the UK. “We have a huge opportunity to learn from countries that have demonstrated expedited or agile ways to ensure safe and fiscally responsible availability of these innovations,” she said. “If we look at those best practices, we can consider what a parallel pathway could look like.”42
References
1. IQVIA Market Access Metrics, December 2024.
2. More than just medicines: Canada’s innovative pharmaceutical industry is contributing to the country’s overall health. Innovative Medicines Canada. Feb. 26, 2024. https://innovativemedicines.ca/newsroom/all-news/more-than-just-medicines-canadas-innovative-pharmaceutical-industry-is-contributing-to-the-countrys-overall-health/
3. Explaining public reimbursement delays for new medicines for Canadian patients. Hoskyn SL, for Innovative Medicines Canada. http://innovativemedicines.ca/wp-content/uploads/2020/06/20200630-CADTH-TTL-Poster-FINAL.pdf.
4. February 2025 Dashboard. pCPA. https://www.pcpacanada.ca/sites/default/files/eng/pCPA_Dashboard_February_2025.pdf.
5. Access and Time to Patient: Prescription Drugs in Canada—January 2024. The Conference Board of Canada. https://www.conferenceboard.ca/product/access-and-time-to-patient-jan2024/.
6. Impact of Trikafta on individuals living with cystic fibrosis. CIHI. November 21, 2024. https://www.cihi.ca/en/impact-of-trikafta-on-individuals-living-with-cystic-fibrosis
7. 20Sense original research.
8. Long wait for cancer drug approvals causing 'great anguish' among patients, doctors. CBC News, January 18, 2025. https://www.cbc.ca/news/canada/ottawa/long-wait-for-cancer-drug-approvals-causing-great-anguish-among-patients-doctors-1.7431786
9. “Why not me?”: Many SMA patients left without access to disease-modifying medicines due to age, geography. Patient Voice. August 16, 2024. https://www.patientvoice.io/many-sma-patients-left-without-access-to-disease-modifying-medicines-due-to-age-geography
10. ‘There’s been a cost put on our child’s head’: B.C. to cut off drug treatment for 9-year-old girl with rare disease. CTV News. Feb.7, 2025. https://www.ctvnews.ca/vancouver/article/theres-been-a-cost-put-on-our-childs-head-bc-to-cut-off-drug-treatment-for-9-year-old-girl-with-rare-disease/
11. B.C. to continue covering 9-year-old’s $1M drug as it reviews cancelled coverage. Global News. Feb. 18, 2025. https://globalnews.ca/news/11024548/charleigh-rare-drug-coverage-update/
12. Ontario 2025 election and take-home cancer drugs. Rethink Breast Cancer. https://rethinkbreastcancer.com/articles/ontario-2025-election-and-take-home-cancer-drugs)
13. Opening Plenary: Introducing Canada's Drug Agency. CDA-AMC Symposium. Sept. 5, 2024, Ottawa.
14. Council of the Federation Fall Meeting, closing news conference. Dec. 16, 2024. https://www.youtube.com/live/Ln2weDvQzxg.
15. pCPA temporary access process. https://www.pcpacanada.ca/pCPATemporaryAccessProcess
16. Success stories. Life Sciences Ontario. https://lifesciencesontario.ca/wp-content/uploads/2024/12/Success-Stories-2024-2.pdf
17. Government of Canada improves access to affordable and effective drugs for rare diseases. March 22, 2023. https://www.canada.ca/en/health-canada/news/2023/03/government-of-canada-improves-access-to-affordable-and-effective-drugs-for-rare-diseases.html
18. Drugs for rare diseases bilateral agreements. Government of Canada. March 13, 2025. https://www.canada.ca/en/health-canada/corporate/transparency/health-agreements/shared-health-priorities/drugs-for-rare-diseases-bilateral-agreements.html
19. 2025: Canada still only developed country with no rare disease plan. Patient Voice. Feb. 28, 2025. https://www.patientvoice.io/perspectives/2025-canada-still-only-developed-country-with-no-rare-disease-plan
20. Beeton activists advocate for rare diseases ahead of Ontario election. Simcoe.com. Feb. 13, 2025. https://www.simcoe.com/politics/provincial-elections/beeton-activists-advocate-for-rare-diseases-ahead-of-ontario-election/article_b23df86b-6f83-5f9f-b9ce-7b211ee4d176.html
21. Letter to the federal party leaders of Canada. CORD. Jan. 14, 2025. https://www.raredisorders.ca/uploads/Letter%20to%20federal%20political%20leaders%20January%202025%20FINAL.pdf
22. Rare Disease Day 2025 webinar. https://www.youtube.com/watch?v=f-PrrHFjyf4
23. Project Orbis. Government of Canada. May 10, 2022. https://www.canada.ca/en/health-canada/services/drugs-health-products/international-activities/project-orbis.html
24. Federal Provincial Territorial Health Ministers' Meeting. Jan. 30, 2025. https://www.canada.ca/en/health-canada/news/2025/01/federal-provincial-territorial-health-ministers-meeting-january-30-2025-halifax-ns.html
25. Caetano T. Innovative Pathways to Reimbursement. CORD Fall Forum. November 2024.
26. Working toward target zero: expanding our rolling review pilot process. CDA-AMC. July 25, 2024. https://www.cda-amc.ca/news/working-toward-target-zero-expanding-our-rolling-review-pilot-process
27. CADTH’s time-limited recommendation category aims to support earlier access to promising drugs. Canada’s Drug Agency. 2023. https://www.cda-amc.ca/news/cadths-time-limited-recommendation-category-aims-support-earlier-access-promising-drugs
28. Wills A. Frontiers. Oct. 7, 2024. https://www.frontierspartnerships.org/journals/journal-of-pharmacy-pharmaceutical-sciences/articles/10.3389/jpps.2024.13694/full
29. Pharmaceutical reviews plan renewal. CDA-AMC. March 6, 2025. https://www.youtube.com/watch?v=hgKxoiTKX3Q
30. Cowling T et al. J Med Econ 2023;26:144. https://www.tandfonline.com/doi/pdf/10.1080/13696998.2023.2237336
31. SPINRAZAMC – Amyotrophie spinale 5q de type II, de type III et présymptomatique. Avis transmis à la ministre en décembre 2018. INESSS. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Janvier_2019/Spinraza_2018_12.pdf
32. Reimbursement recommendation – nursinersen (Spinraza). CADTH. August 2022. https://www.cda-amc.ca/sites/default/files/DRR/2022/SR0713-Spinraza-Reassessment.pdf.
33. Tisagenlecleucel pour le traitement du lymphome diffus à grandes cellules B récidivant ou réfractaire. INESSS 2019. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Therapies_cellulaires/INESSS_Avis_Kymriah_LDGCB.pdf
34. Axicabtagene ciloleucel pour le traitement des lymphomes à grandes cellules B récidivants ou réfractaires. INESSS. 2019. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Therapies_cellulaires/INESSS_Yescarta_Avis_Cav.pdf
35. KYMRIAHMC – Lymphome à grandes cellules. Avis transmis au ministre en mai 2024. INESSS. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Juin_2024/Kymriah_LGCB_2024_05.pdf
36. YESCARTAMC – Lymphome à grandes cellules. Avis transmis au ministre en mai 2024. INESSS. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Juin_2024/Yescarta_2024_05.pdf
37. Benoit A. Clin Lymphoma Myeloma Leuk 2023;23:203-210. https://pubmed.ncbi.nlm.nih.gov/36646606/
38. Avis transmis au ministre en mai 2024. INESSS. https://www.inesss.qc.ca/fileadmin/doc/INESSS/Inscription_medicaments/Avis_au_ministre/Juin_2024/20240506_AvisMinistre.pdf
39. Marando D. Canadian health care’s biggest ailment? Tidy narratives. Healthy Debate. Nov. 26, 2024. https://healthydebate.ca/2024/11/topic/canadian-health-cares-ailment-reform/
40. Collaborative solutions to timely patient access to cancer treatments. Life Sciences Ontario. November 2024. https://lifesciencesontario.ca/wp-content/uploads/2025/01/25-01-14-TPP-session-summary-v6.pdf
41. Villalba E. LinkedIn post. March 11, 2025. https://www.linkedin.com/posts/evavillalba1_h%C3%B4pital-pierre-legardeur-des-d%C3%A9lais-d-activity-7304950993652240386-jM1I
44. Innovative partnership aims to offer less invasive cancer treatment for New Brunswick patients. Roche Canada. https://www.rochecanada.com/media/innovative-partnership-aims-to-offer-less-invasive-cancer-treatment-for-new-brunswick-patients.
45. Innovative partnership will deliver expedited access to cancer treatment for New Brunswick patients. Horizon Health Network. https://horizonnb.ca/news-releases/innovative-partnership-will-deliver-expedited-access-to-cancer-treatment-for-new-brunswick-patients/.